Part 5! Today we’ll delve into the last of the six archetypes, The Transcender.
Before we start, I’d just like to clarify that I am not claiming to be a Transcender. Far from it. I struggle daily with my Exerciser tendencies (I’m pot nerfect and I have them). I try my best to be aware of the pull of Over-Identifier-ing. I like to think I possess some of the healthy balanced qualities of The Integrator, but fall short on many occasions. Most days, if I’m lucky, I am able to remember how I aspire to cultivate Transcender qualities. Just remembering is hard (and this is where mantras, in a non-fluffy, practical way come in handy. But more on that later).
The only reason I feel authorized to write about The Transcender archetype is that I have a few mentors in my life that I would describe as such. I’ve been fortunate to spend time with these individuals, seeing how they live their lives over the course of a day, how they think and behave, and the congruence between the two. Observing what they value, what their priorities are, how they interact with their bodies.
It is because of these people that I feel capable of writing this chapter. I hope you’ll be as inspired by this archetype as I have been by The Transcenders I am lucky to know and learn from. Making the time to thoughtfully write down this description was a gift: The reflecting on what qualities and traits these inspiring people have was illuminating. What is it exactly about these people that makes it feel so different to be with them?
Complementarity: A Principle to Live By
The Transcender was a difficult character for me to pin down (also one of the reasons I am writing about him last). To nail his description, I think it is necessary to first discuss the concept of complementarity.
Complementarity is a principle from the weird world of quantum physics developed by Neils Bohr, a leading founder of the field. It states that to understand one entity or phenomena in its entirety, we may need to understand it broken down into two or more mutually incompatible theories. It speaks to the complexity, uncertainty, and indeterminacy of things. Things that have complementary properties which cannot all be observed or measured simultaneously.
A prime example of complementarity in physics is that we cannot simultaneously observe wave and particle properties. Nor can we measure position and momentum at the same time with the same instruments. The stage we’re in now, as a technological species, it is not possible to conceive of or measure properties inherent to the thing in question beyond what is possible with our specific measuring tool: The type of measurement determines which property is shown. In essence, it is near impossible to see the whole truth of a thing through one lens. It only seems possible to garner some semblance of understanding of a thing by reducing it to multiple, contradictory parts, then putting the pieces back together again.
I am enchanted with how complementarity not only describes an aspect of the fabric of reality, but how it can serve as a useful way of perceiving the world and living in harmony with it at an individual level.
If The Transcender had a religion, he’d be a Complementarian. This was a conclusion I came to after listening to an interview with physicist Frank Wilczek on Krista Tippett’s radio show On Being, in which he laid claim to this as his own religious belief (only half jokingly). To him , complementarity wasn’t just a physical principle, but a way of living. He described how he takes his understanding of complementarity and its application in physics into his daily interactions with people and the world around him.
In Wilczek’s words, the practical application of complementarity is based on the recognition that “a deep truth has the feature that its opposite is also a deep truth”. That there are different ways of viewing the world and we need both and all if we want the complete picture, as each is valid in its own context.
Just as we can observe matter organized as a particle or a wave depending on what instrument we are measuring it with, our interpretation of human behaviour, thoughts, and feelings will depend on our lens, context, and reference point of observation. Thoughts and feelings are about as mutually incompatible as particles and waves, and only rarely can we view them together as a coherent whole with any clear understanding of what’s really going on.
What makes complementarity useful for us (other than that it is an organizational principle of reality on the micro scale which it would seem foolish not to want to investigate in the macrosphere we interact in daily), is, as Wilczek explains, “It is interesting, fun, and informative to appreciate there are different ways of viewing things that each have their own validity, but conflict if you try to apply them both at once. Apply one at a time and try to appreciate both.”
His belief, one that I feel to be an astute observation, is that there is virtue and intelligence in being able to live with this uncertainty and inconsistency, that this is an important component of wisdom.
This wisdom, this appreciation of multiple views and ways of thinking and doing all as valid in their context, is the primary defining trait of The Transcender.
The Transcender
The Transcender’s mantra could be taken directly from Nassim Nicholas Taleb’s book, Antifragile: “I want to live happily in a world I don’t understand”. He has a love for the uncertain. He is curious about inconsistencies. He is a seeker of truth.
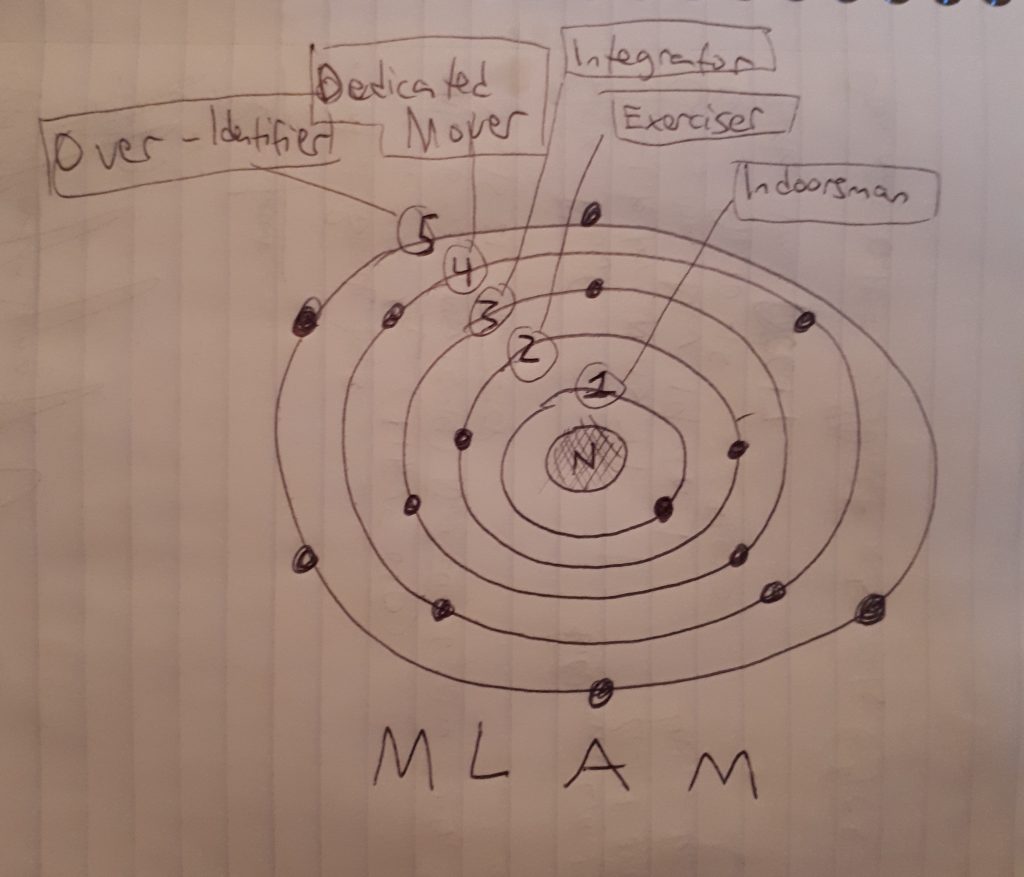
In our MLAM, The Transcender cannot be confined to a single shell. As a Complementarian, he he is able to jump from shell to shell at any given moment based on the dictates of context: His present needs and goals. He is the model in its entirety, without being attached for too long to any of the archetypes he inhabits. He appreciates how the traits from each archetype serve a purpose that is useful. He can only be fully understood as a whole by understanding the other five archetypes and their ways of living.
The Transcender is rare, but it is likely that you can identify at least one in your life. He is probably someone you admire and look to as a role model. Someone to learn from.
Movement is one of The Transcender’s highest values, but to him movement goes beyond physical exercise (we will look at this broader definition of movement in the next chapter). He sees movement in its every form in nature and is fascinated by it, its reflection and representation and in our lives. For example, how the movement of the seasons mirror the movement of our thoughts, the function of our bodies. His overarching view of movement as seasons, cycles, and patterns, as a fundamental property of everything, explains how he is able to maintain his value for movement at all times while himself being in a sedentary character.
The Transcender is excellent at recognizing patterns and appreciates that his life happens in cycles of complementarity: Cycles of input and output, activity and non-activity, introspection and extroversion, play and rest, etc. He also acknowledges that these cycles may last moments, days, years, or decades, and is perfectly comfortable with that. These patterns are only recognizable with a sufficient amount of time and introspection, and so the Transcender is likely to be at least 30 years or older- Enough time to experience the validity of each cycle in its current context. This understanding is what makes him peaceful to be around. He isn’t fighting the currents of his life, but flowing with them.
In more practical terms, on any given day The Transcender can adopt the characteristics of any of the other archetypes but without becoming stuck in any of their patterns.
For example, The Transcender may have led the highly active life of a Dedicated Mover for 10 years as a professional cyclist, but then out of necessity (a signal to rest such as an injury, or a change in priorities) become a bit of an Indoorsman, deciding to commit his next five years to writing a book he felt compelled to bring to fruition based on these 10 years of lessons as a cyclist. He makes use of The Indoorsman archetype’s characteristics, rather than allowing The Indoorsman making use of him. This is the key distinction between The Transcender in Indoorsman’s clothing, and a true Indoorsman. He play’s The Indoorsman character without carrying these characteristics into other areas of his life in which they won’t serve. It is as if he can put on the costume of an archetype, and change out of it to play the role necessary for the next act of his life, whether it lasts for 5 minutes or 20 years. One of his superpowers is adaptability.
While he is capable of stepping in and out of the shoes of The Indoorsman and Exerciser (two of our archetypes with the least healthy relationships with movement), he was probably encouraged in his childhood to always be moving, playing, and being outdoors, values that stuck with him. As the driving force in his life is his curiosity about movement, most things he deems a good use of his time involve learning about, practicing, or deepening his understanding of the human body in motion. He considers himself a life-long student of movement, and he studies via books and taking courses, experience working with other people, but perhaps most importantly, exploring in his own body, developing a deep awareness of it.
What he knows to be true through his own experience studying his body in motion is that what he observes to be happening in his body also shows up in his life. When he feels resistance and limitation in his body, somewhere in his life he knows this same restriction must exist and he seeks to understand this connection. To him, the exploration of his body is a vital, inextricable part of investigating his life and how he interacts with it. He knows that his relationship with his body and how it moves- what’s going on “in here”, is a reflection of what’s going on “out there”. This is not something he can prove scientifically, but witnesses again and again in himself and the lives of others. This insight makes him sought after for advice. Being with him in is like taking a ride in a helicopter from which we can view a greater expanse of the landscape of our lives. To zoom out and see a fuller picture of reality.
As much as he values and loves moving his body, he is equally able to be with himself in stillness. He can sit down to meditate, scan his body, or to read or write or study for hours. Another one of his amazing super-powers is his resiliency to sitting. Immobilization in front of a computer or on a plane don’t have much of a negative long term effect (not that he enjoys these things exceptionally). He simply stands up, shakes off any feelings of crustiness, and gets on with life with no excuses, regrets, or procrastination, like many of us are prone to do.
It is his commitment to learning about and from himself, his body, and the world around him that define the core intention of The Transcender’s movement practice. In his quest to satisfy his curiosity, he is likely to develop a propensity for teaching, allowing him to share what he is learning and exploring, while deepening his understanding of himself and the human body. Likely career paths for him thus include coaching a sport or movement form, working as a therapist of some designation, teaching seminars, or authoring a book (or all of the above at different life-stages). His ability to play all parts in MLAM serves him nicely in these guiding roles, endowing him with an easy sense of compassion and drawing his “tribe” to him in his capacity as coach, teacher, and healer.
The Transcender is distinguished from the Dedicated Mover and The Over-Identifier by his realization that he cares more to explore, tinker, play, and teach than to compete, win, and be the best. He may have transitioned from being a serious athlete to his teacher/coach/healer role with the understanding that while he loves that particular sport, he gives precedence to having a healthy body and mind, a goal requiring a more diverse movement “diet”, not to become stuck in one pattern.
As his name suggests, The Transcender transcends the need to always be moving: He doesn’t obsess about his training schedule, doesn’t feel guilty for missing a training session, doesn’t succumb to the pressure to exercise because “he should”. He knows to rest when things don’t feel right in his body. He fluctuates between moments of deep focus, relaxation, or calm, and bouts of intense activity, skilled practice, or inspired teaching. Because of this, he is in good physical health much of the time (though he comes in different shapes and sizes).
It is as if his MLAM shell-position operates on a highly sensitive pressurestat* system allowing him to adapt to each moment in time appropriately. For example, if he stops moving for long enough, his inner homeostatic mechanism signals a build up of pressure and cues him to get up and move. And when his system needs a break to recover (low pressure) the signal is heeded; he slows down and enjoys some downtime. This happens at both the micro (seconds, minutes, days, weeks) and macro (months, years, decades) level. He rarely needs to think long and hard about what is best for his body, he is adept at interpreting his inner-pressurestat’s readings.
*A pressurestat is a homeostatic control that reacts to changes in pressure in a system, increasing or decreasing it according to the environmental conditions.
This ability to clearly communicate with himself is mirrored back at him in his relationships and professional life. The Transcender tends to have clear, intact boundaries, knowing when to say “no” or “yes” to himself and others in personal and professional matters. Rarely does he burn himself out, as his internal feedback loop provides accurate real-time information on when to stop, go, or change lanes. That said, he has developed a particularly low tolerance for irrational thinkers, from whom he has learned that life is too short to live trying to convince them of their irrationality or change their minds.
Finally, an interesting characteristic of The Transcender is that he may not consider himself to even have a movement practice, even if it appears to the outside eye that he does. If you ask him about it, he doesn’t feel that he is practicing anything, just that he is living his life authentically according to his values and priorities. In this way, The Transcender effortlessly takes on a teaching role by virtue of modeling how to live a life in congruence with one’s highest values.
The Transcender at a glance:
Superpowers: Resilience to sitting, adaptability, curiosity, teaching, communication.
Religion: Complementarian
Kryptonite: Irrational thinkers.
Vitality: Healthy, abundance of energy, youthful.
Relationship with movement: Transcendent.
Attitude towards the stairs: Take em’ or leave em’, depends on his pressurestat.
Identify with the traits, not the character
As I mentioned before, these archetypes are stories. Communication devices to frame the rest of what I wish to discuss in this work.
You can probably identify some traits from each archetype in yourself, or maybe fully identify with one of them. Perhaps you have an idea about aspects of your archetype that you are unsatisfied with, that you’d like to change. But I’d also like you to ask yourself, how are these undesirous traits currently serving you, where you are now in your life?
Put on The Transcender’s thinking cap, or take a ride with him in his helicopter. Can you see the broader landscape of your life?
A conversation between an Exerciser and a Transcender from up in his helicopter might look like this.
Exerciser: After reading Monika’s description of The Exerciser archetype, I can see how I use exercise as a way of making up for my unhealthy habit of neglecting my body all week as I work at my IT job at Clean Clean Happy Time Toilets and Bidets Inc. I’m unhappy that this is a trait I possess.
Transcender: Let’s zoom out and investigate this. Can you see ways that this undesirable trait is actually useful for you? What could it be helping you to accomplish and learn? Who else could be benefiting from it? How would you feel if you could let go of this trait, and What would you do with the space you’d free up without this trait as part of your existence?
Your first exploratory mission
Consider this your first step in our systematic approach to cultivating a healthy, useful, enjoyable movement practice.
Exercise 1:
I’d like you to take the imaginary ride with The Transcender described above. Start by writing down some of the characteristics you identified with from each archetype (there will probably be some from each). Go back and re-read the descriptions if necessary. Then, for each characteristic, write down your answers to these six questions:
1. How is this undesirable trait useful for you?
2. What could it be helping you to accomplish?
3. Who else could be benefiting from it?
4. What have you learned from being this way?
5. How would you feel, who would you be, if you could let go of this trait?
6. What would you do with the space you’d free up in your life without this trait as part of your existence?
Doing this reflection and writing down your answers is an illuminating use of time, and I strongly recommend you do it. It will help to give clarity to your “now”, which, at some point will likely be your “then”.
Practical post-archetype semantics
The next chapter of this work will describe and define some important words, like movement, practice, and exercise, so that you, where ever you sit on the MLAM, can gain a fuller understanding of the role movement plays in our lives, and how to cultivate healthier relationships with our bodies on this journey of well-being*. The more you are aware of where you are now on the MLAM by investigating your archetypal ways of living, the more you will appreciate the chapters to follow.
*Well-being: I believe it is impossible to define and measure objectively because it a journey, not a fixed state.
 *A Black Swan (referring to the bird, not he ballet), as described in the book by the same name by the statistician and former trader Nassim Nicholas Taleb, is a rare, unpredictable event (good or devastating). Those who know they cannot predict a Black Swan event, but recognize the potential for one are at an advantage as they are able to bolster themselves against the devastating effects should one happen. However, those who are most susceptible to a Black Swan are those who think they can predict the future, think bad things can’t possibly happen to them, and ignore the potential risk because it is so small. For example, if you live in Seattle, a city on a fault line, you are at risk at any time for a massive earthquake to destroy your home. This earthquake is a Black Swan event- A rare, unpredictable event that is impossible to protect against completely. It may happen tomorrow, it may not happen in your lifetime. But it is possible to minimize its catastrophic impact on you by knowing about its potential impact. Bolstering against the earthquake could include a. Moving away or living only a few months of the year in Seattle, b. Educating yourself on safety procedures should there be an earthquake, c. Not owning anything that you know you would hate to lose, etc. None of these are perfect- There is no perfect protection from a Black Swan by its very nature, but with our knowledge that one is possible we can minimize our fragility to one.
*A Black Swan (referring to the bird, not he ballet), as described in the book by the same name by the statistician and former trader Nassim Nicholas Taleb, is a rare, unpredictable event (good or devastating). Those who know they cannot predict a Black Swan event, but recognize the potential for one are at an advantage as they are able to bolster themselves against the devastating effects should one happen. However, those who are most susceptible to a Black Swan are those who think they can predict the future, think bad things can’t possibly happen to them, and ignore the potential risk because it is so small. For example, if you live in Seattle, a city on a fault line, you are at risk at any time for a massive earthquake to destroy your home. This earthquake is a Black Swan event- A rare, unpredictable event that is impossible to protect against completely. It may happen tomorrow, it may not happen in your lifetime. But it is possible to minimize its catastrophic impact on you by knowing about its potential impact. Bolstering against the earthquake could include a. Moving away or living only a few months of the year in Seattle, b. Educating yourself on safety procedures should there be an earthquake, c. Not owning anything that you know you would hate to lose, etc. None of these are perfect- There is no perfect protection from a Black Swan by its very nature, but with our knowledge that one is possible we can minimize our fragility to one. 

 Concurrently to this story about L, I was reading John Upledger’s The Inner Physician and You in preparation for taking the Upledger Institute’s craniosacral therapy level one course (stoked!). Reading this book was fortuitously timed, as I began to observe some of its main themes surface in my bodywork practice. In particular while working with L last week.
Concurrently to this story about L, I was reading John Upledger’s The Inner Physician and You in preparation for taking the Upledger Institute’s craniosacral therapy level one course (stoked!). Reading this book was fortuitously timed, as I began to observe some of its main themes surface in my bodywork practice. In particular while working with L last week.